Normal Lung Ultrasound
This lesson will cover the standard locations for lung ultrasound and the normal findings in those locations.
Probes and settings to use:
- any probe can be used in the anterior position
- if focusing on the pleural line, then a depth of 6 cm should vertically center the pleura on the screen
- the cardiac (phased array) or abdominal (curved array) probe must be used for posterior or lateral positions because the required depth is too much for the vascular probe
Scanning Locations:
- The patient may be examined in a seated or supine position
- A seated position is usually easier for assessment of the posterior thorax
- The probe is oriented in a longitudinal orientation (probe marker pointing to the head)
- The thorax must be examined in a systematic manner to look at all lung regions
- Different lung scanning protocols have been described
- Two common protocols are presented: the "BLUE points" and the Volpicelli method
- Superiority of one specific protocol has not been demonstrated
- The examiner should take care to ensure the ultrasound probe is positioned exactly perpendicular to the pleura to maximize pleural line echogenicity and generated artifacts.
The “BLUE Points” Method
- Identify four anatomical points on each hemithorax (there will be a total of 8 points with both lungs).
- Point 1: upper anterior chest wall, 2nd rib space, mid clavicular line.
- Point 2: anterior axillary line, 5th rib space (nipple line). This examines the middle lobe on the right side.
- Point 3: mid-axillary line at the level of the diaphragm.
- Point 4: is the PLAPS (posterolateral alveolar or pleural syndromes) point immediately posterior to point 3. Press the probe as posterior as possible into the bed while maintaining a perpendicular orientation to the skin.
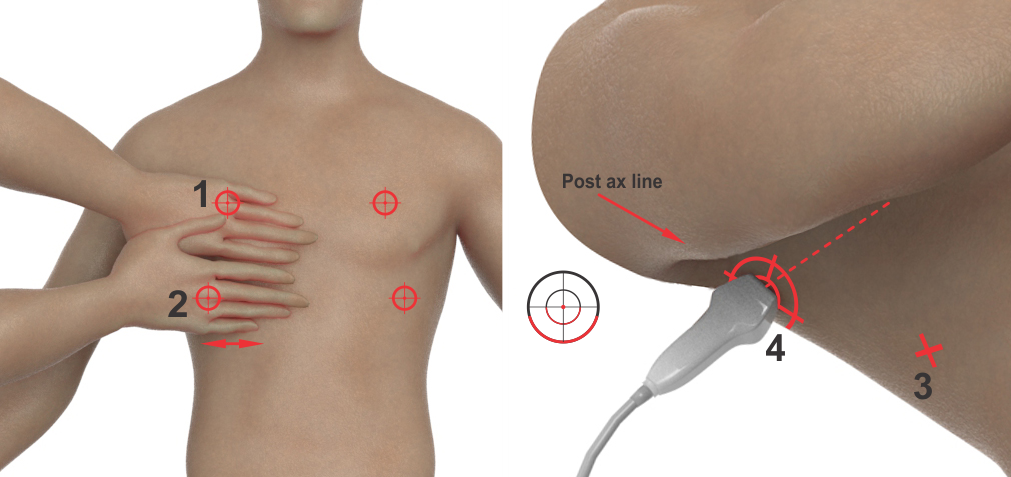
Figure 4. Blue Points. Image modified from Lichtenstein, et al.1
The Volpicelli method: this is similar to the Blue Points, providing 4 zones, each requiring a single examination region on each hemithorax, for a total of 8 points for a full thoracic exam.2
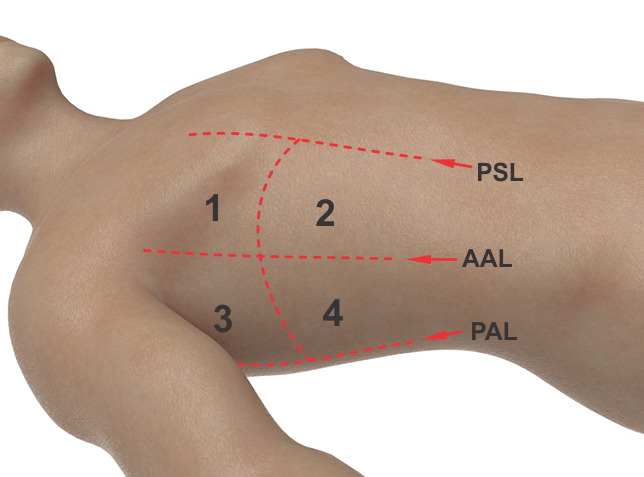
Volpicelli protocol with 4 areas in each hemithorax. Taken from Volpicelli, et al.2
PSL = parasternal line
AAL = anterior axillary line
PAL = posterior axillary line
Normal Appearance, Anterior Scanning Location: scanning depth should be 10-12 cm. but can be much less too (image below is 4 cm deep)
The top (superficial) portion of the image will consist of fat, muscle and bone (the chest wall).
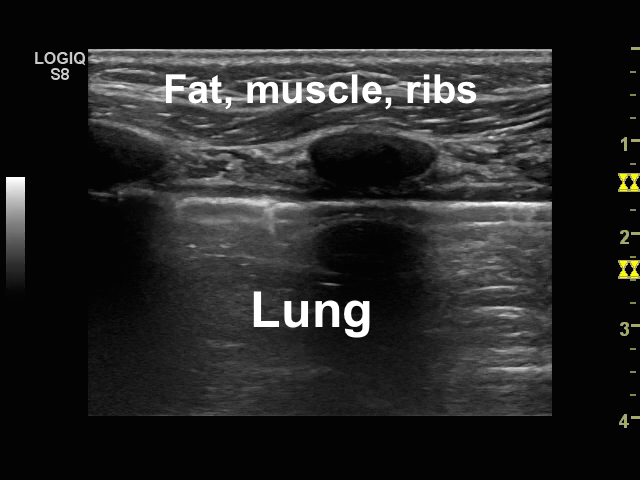
The pleural line is very important to identify:
.png)
The ribs will cast shadows. These are artifacts. The rib shadows are outlined by the yellow lines below:
.png)
Many ultrasound images look like other imaging. Here, you can see that a CT of the heart can look very similar to an ultrasound. Tissue looks like tissue and chambers look like chambers:
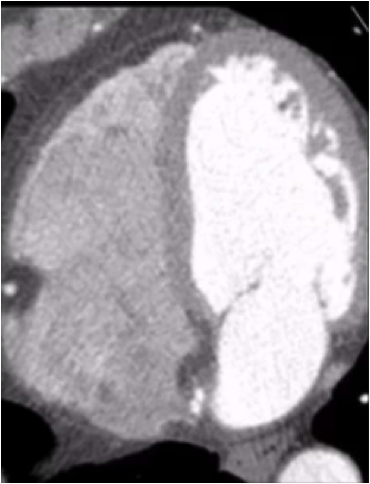
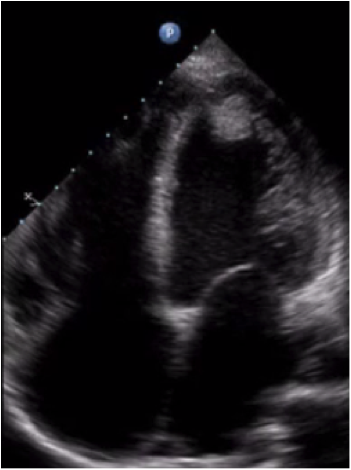
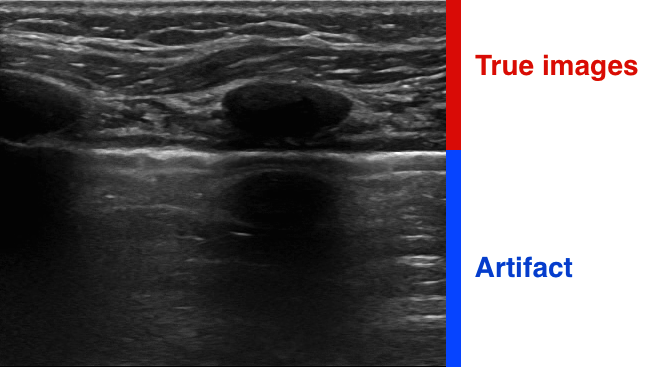
Lung ultrasound is different and is about artifact analysis. Air does not transmit ultrasound waves. It will scatter them.
As a result, EVERYTHING we see below the pleural line "inside" the lungs is artifact (bottom blue zone). Can you see a "fake" mirror image of the ribs inside the lung? Everything we see above the pleural line are true images of muscle, fat and bone.
Lung Sliding
- lung sliding is a normal finding and should be observed
- requires the visceral pleura to be moving relative to the parietal pleura
- requires these 2 pleural surfaces to be in contact with each other
- relative to the ultrasound probe, the chest wall does not move, but the lung does
- the lung can be seen moving left and right with inspiration and expiration
Here is a video example of lung sliding:
Absence of lung sliding occurs when:- the 2 pleural surfaces are not in contact with each other:
- pneumothorax
- pleural effusion
- the lung is not moving relative to the chest wall:
- the lung is adherent to the chest wall
- the portion of lung that is imaged is not being ventiltated
- endotracheal tube is in contralateral bronchus
- lung is full of pus (severe pneunomia)
- advanced bullous COPD
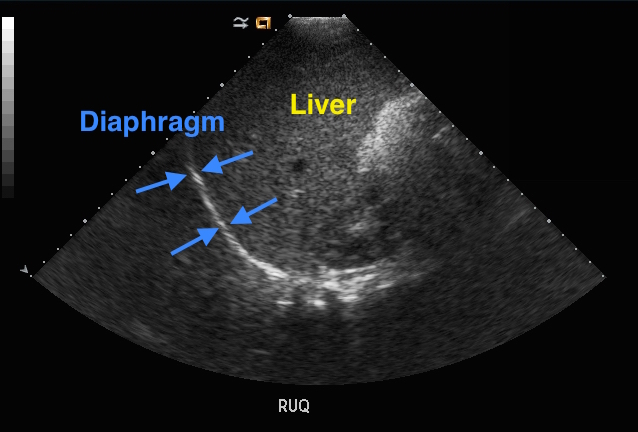
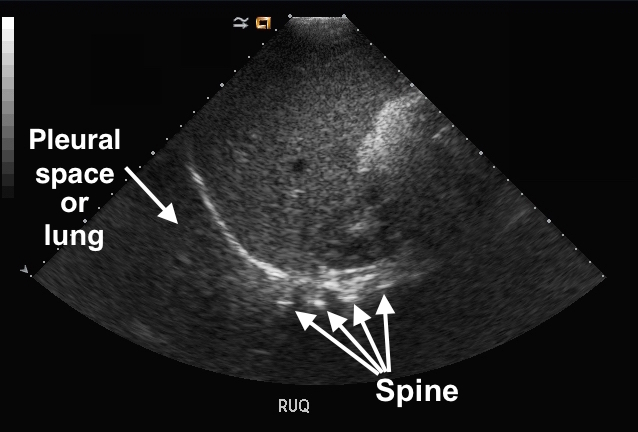
Normal Appearance, Posterior and Lateral Scanning Locations:- scan depth should be 14-16 cm
- scanning in the posterior zone needs to include the diaphragm
- on the right, the liver will be seen below the diaphragm
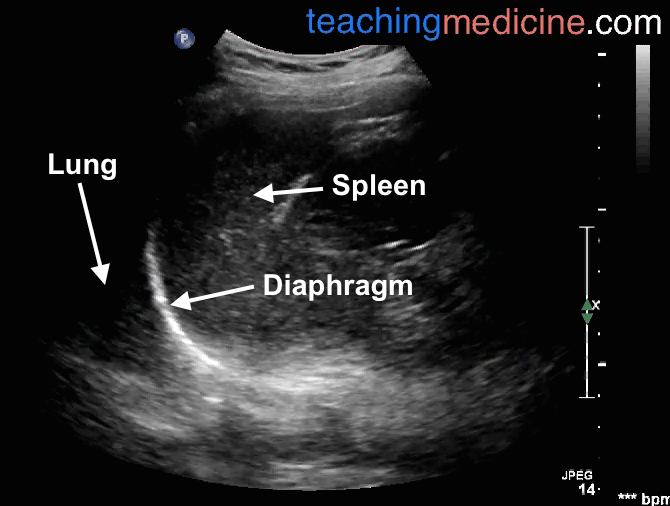
- one the left, the spleen will be seen
- kidneys will may be visible as well
- the spine can also be visualized at deeper depths
The images below are taken from the patient's right side, so the liver is seen:
The image below is from the patient's left side, showing the spleen. The spleen and liver are similar (but not identical) in appearance:
Summary of normal lung ultrasound:
- use an organized approach to view 4 locations on each lung
- anterior view must highlight the ribs and pleural line
- posterior views must highlight the diaphragm and liver/spleen
- all images "inside" the lung are artifact
- sliding lung is a normal finding
References
- Lichtenstein D, Mezière G., (2011). The BLUE-points: three standardized points used in the BLUE-protocol for ultrasound assessment of the lung in acute respiratory failure.Crit Ultrasound J. 24, pp.109-110
- Volpicelli, G. et al., (2012). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 38, pp.577-591
