When the left ventricle becomes hypertrophied, it thickens and develops some degree of fibrosis. The increased mass of the LV results in a stronger electrical signal, having greater voltage. Remember that voltage on the ECG is measured in the "up and down" direction. Therefore, greater voltage results in taller or deeper waveforms on the ECG.
A second effect is that the conduction through thicker myocardium requires more time. Therefore, the QRS in LVH is sometimes increased. Fibrosis could also contribute to slower conduction, and this would also contribute to a wider QRS.
A third effect relates to the ST segment and T wave. Remember that abnormal depolarization usually also results in abnormal repolarization. Therefore, LVH is commonly associated with an abnomal ST segment and T wave.
There are MANY different diagnostic criteria for ECG LVH. In fact, there are 27 different diagnostic criteria listed in the 2009 chamber enlargement guidelines1. Some of the criteria use only limb leads, some only precordial leads, and some use a combination of both limb and precordial leads. Current evidence does not indicate if some diagnostic criteria are superior to others, or if they are simply redundant.
To simplify, all criteria measure the height or depth of the QRS and if these values are big, then LVH is diagnosed. The differences between all the different diagnostic criteria are the selection of ECG leads and the value that is selected.
The electrical vector for the LV (yellow arrows) travels mostly AWAY from V1,2 and mostly TOWARD V5,6: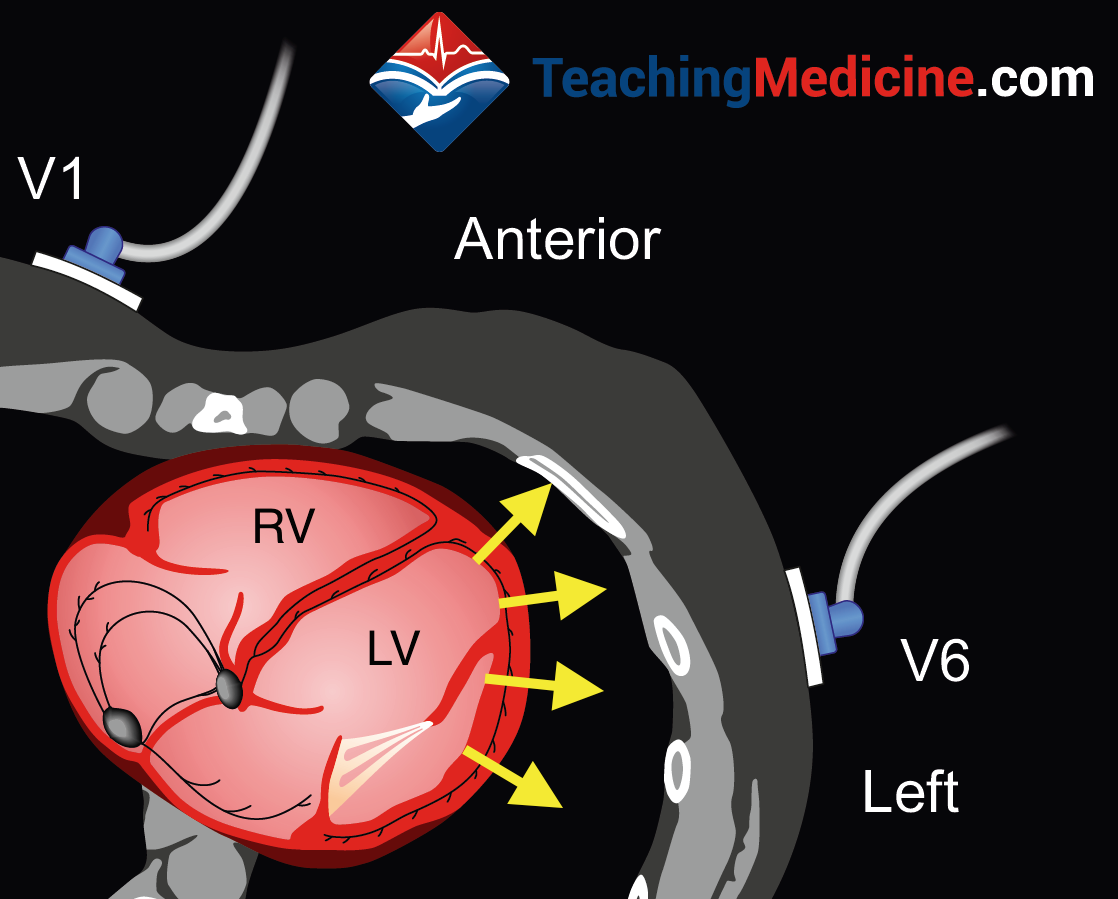
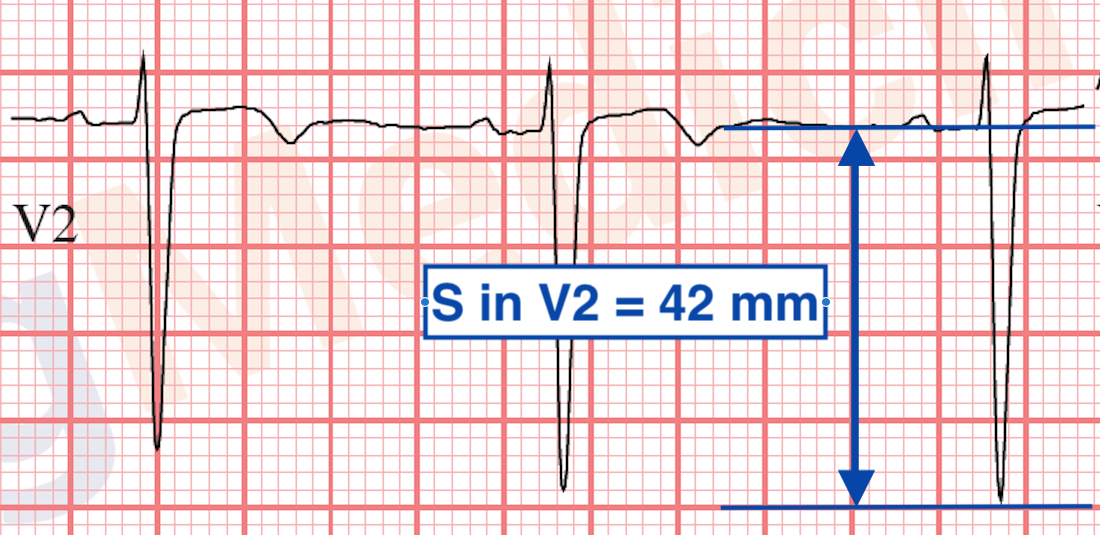
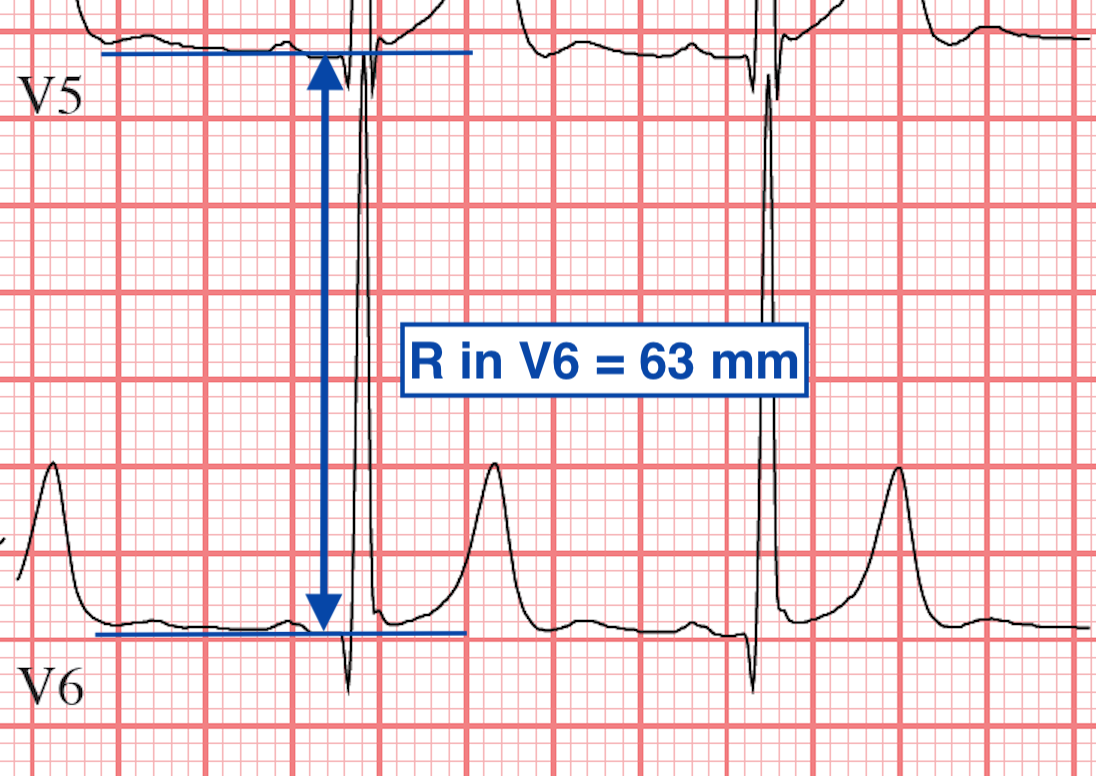
In LVH, the S waves in V1/2 and R waves in V5/6 are amplified. We measure them to see exactly how amplified they are. Here are examples of a deep S wave in V2 and a tall R wave in V6:
Although there are at least 27 sets of criteria, we will present only 3 of them. Only one set of criteria need to be met to make the diagnosis.
"Sokolow and Lyons Criteria"
Use the larger of V5 or V6.In this example, the S wave in V1 = 24 and the R wave in V5 = 42 and total = 66, so criteria is met.
"Cornell Criteria"
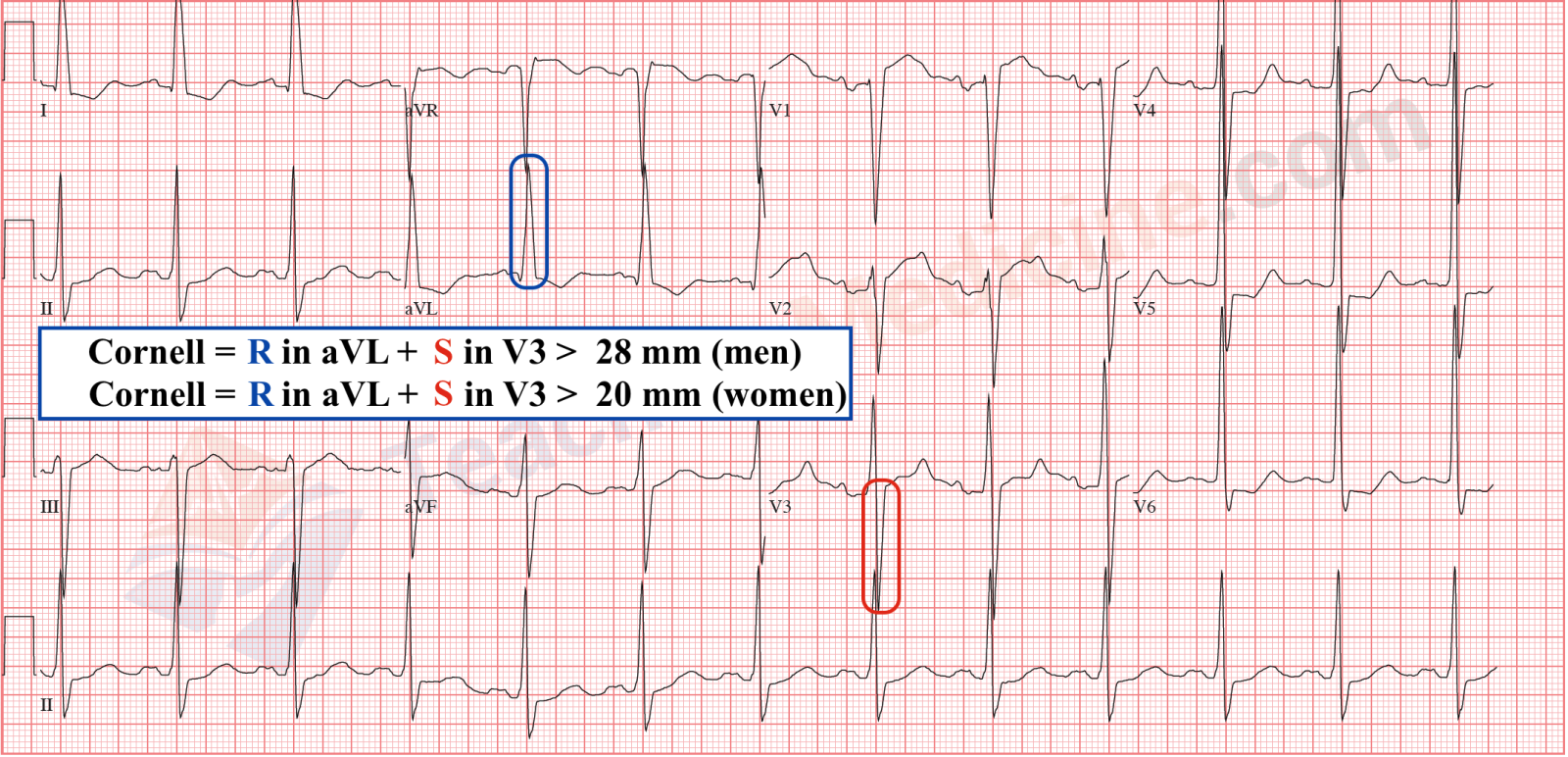
In this example, the R in aVL = 20 and the S in V3 = 20 for total of 40 mm, so criteria is met for either a man or woman.
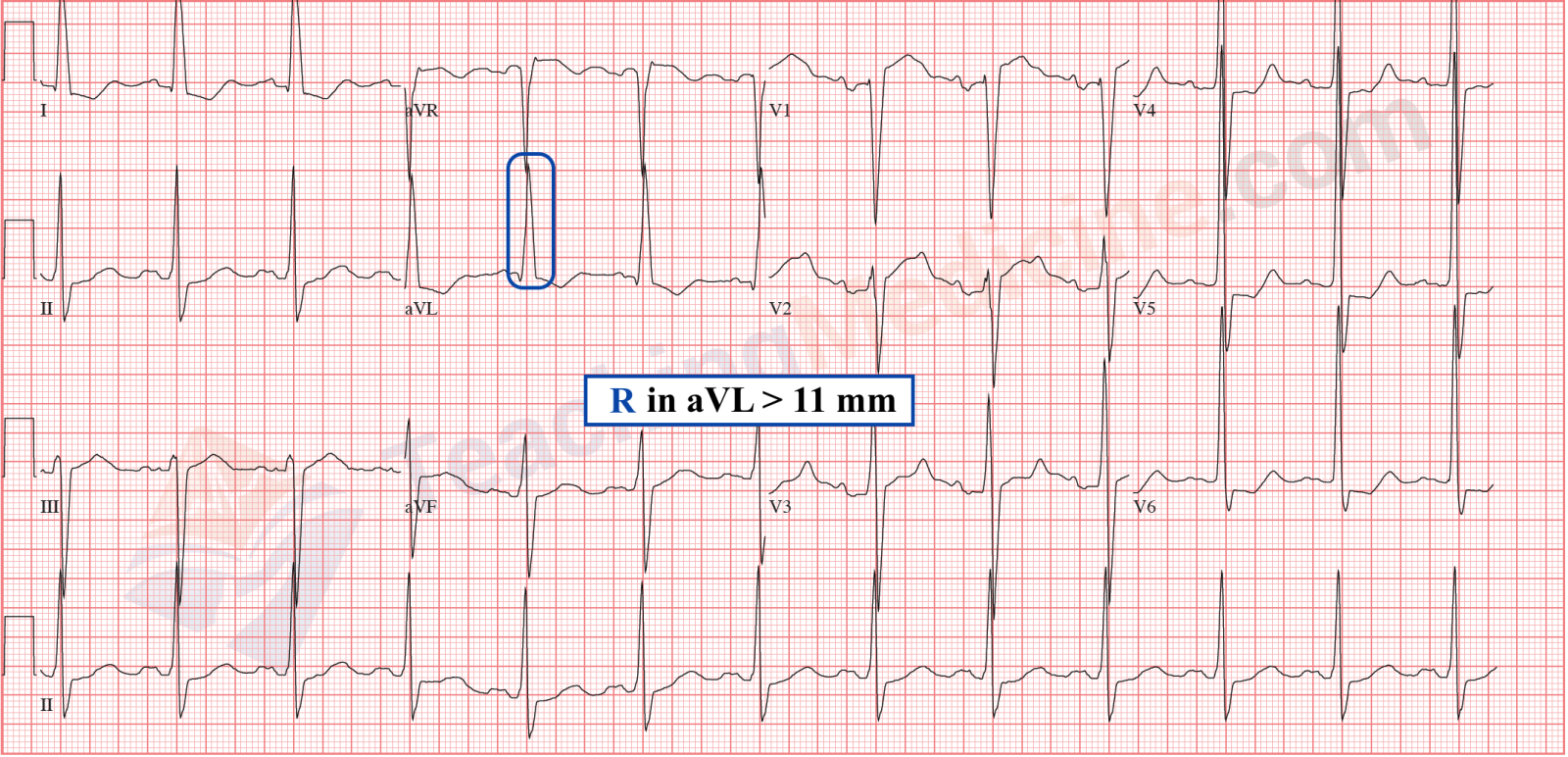
"aVL Criteria" (also by Sokolow and Lyons)
There are other diagnostic criteria that are not listed here. Every set of criteria has a slightly different sensitivity and specificity when compared to echocardiography or autopsy criteria for LVH and no single criteria has yet been demonstrated to be superior.
ST and T wave Changes:
When LVH is present, the ST and T waves are often abnormal. A term called "LVH strain" was commonly used to indicate that there was additional strain on the myocardium resulting in changes in the ST segment and T waves. The AHA recommnedations promote the use of the term "LVH with secondary ST-T wave abnormalities" instead of "strain"1.
The ST and T wave changes are important to identify and characterize because they can cause diagnostic interference with ischemia and infarct (which also cause ST and T wave changes).
There are 3 important "typical" features of ST-T wave abnormalities that are secondary to LVH include:
#1) The ST segment depression/elevation will typically be in the opposite direction to the QRS:The blue arrows indicate ST elevation and upgoing T waves which are associate with downgoing QRS.
The red arrows indicate ST depression with downgoing (biphasic) T waves with upgoing QRS.
#2) The magnitude of ST changes will be proportional to the size of the QRS.
Really tall or deep QRS's will be associated with greater amounts of ST segment depression or elevation.
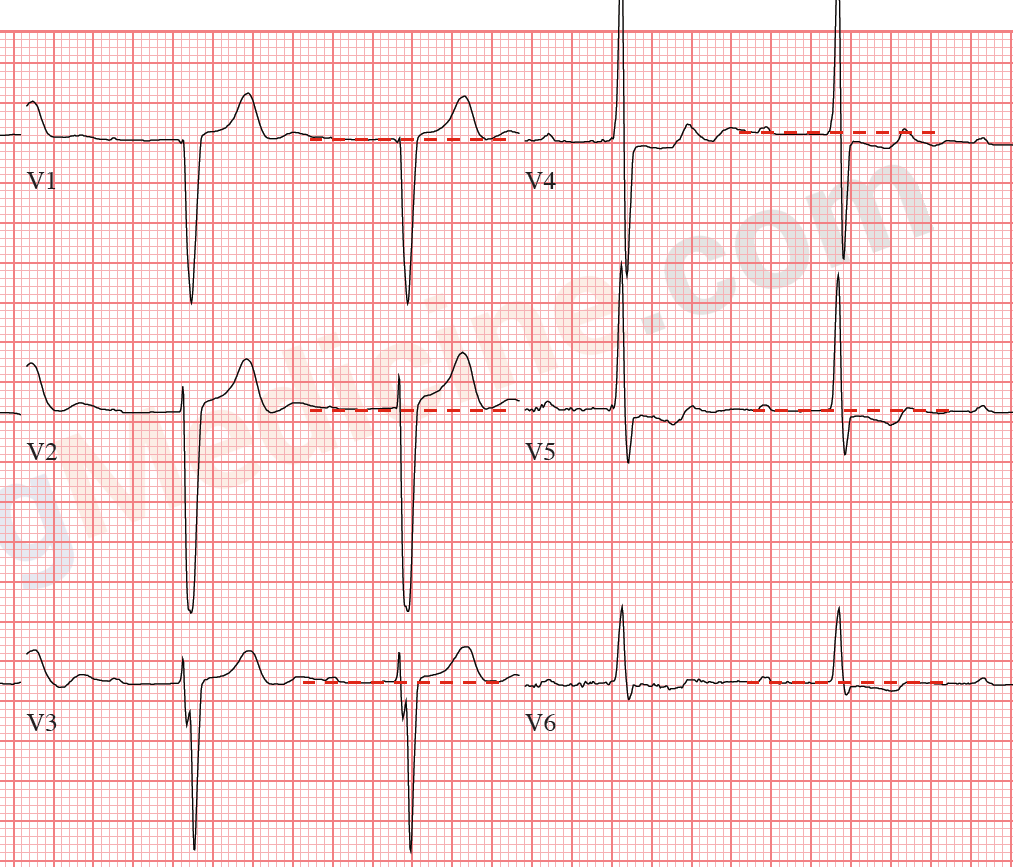
Red dotted lines indicate the isoelectric baseline.
ST elevation is seen in V1-3, greatest in V2 where the QRS is largest.
ST depression seen in V4-6, greatest in V4 where the QRS is largest.
#3) The ST segment will be concave AWAY from the QRS. In other words, ST segment elevation will be concave "upwards" and ST depression will be concave "downwards". 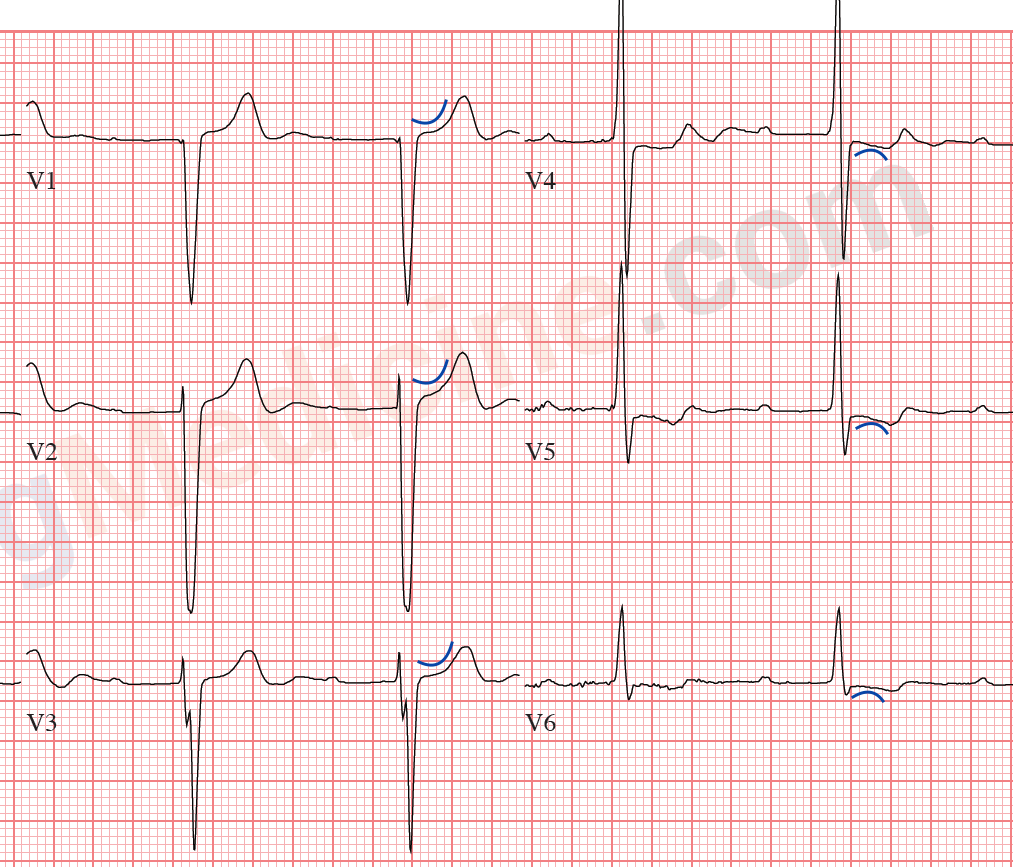
ST segments are concave upwards in V1-3.
Less obviously, are concave downwards in V4-6.
ST changes in LVH vs. Ischemia or Infarction
With myocardial ischemia or infarction:
- ST segments will be flat(ter) and not concave
- ST elevation or depression is not related to the direction of the QRS
- ST elevation or depression magnitude is not proportional to the magnitidue of the QRS
Summary of diagnostic criteria for LVH:
- voltage criteria:
- S in V1/2 + R in V5/6 > 35 or
- R in aVL > 11 or
- R in aVL + S in V3 > 20 (women) or > 28 (men)
- ST segment changes typically will show:
- ST segment deviation away from the QRS
- ST segment deviation is proportional to size of QRS in that lead
- ST depression will be concave away from the QRS in that lead
Increase your diagnostic accuracy: the following features are not required for the diagnosis of LVH, but if they are present, they increase the specificity of your diagnosis (in other words, make it more accurate):
- left atrial enlargement (LAE)
- ST and T wave changes
- a wide QRS
- slightly prolonged QT interval
- left axis deviation
In other words, an ECG that demonstrates voltage criteria plus LAD, ST - T wave changes, and LAE is more likely to be "truly LVH" compared to an ECG with the same voltage criteria without those extra features.
1. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram Part 5. JAC. 2009;53(11):992–1002. doi:10.1016/j.jacc.2008.12.015.
