Right Ventricular Hypertrophy
The diagnosis of right ventricular hypertrophy (RVH) can be made on ECG. However, the diagnostic criteria are not particularly sensitive nor specific. This means that diagnosing RVH on ECG using a set of criteria will result in some cases of RVH being missed and some cases of RVH being diagnosed when it is in fact not present.
Echocardiography is a better test to diagnose RVH, but ECG does have value.
To make matters a little bit more complicated, RVH usually occurs in the presence of other pathologies and these other pathologies can interfere with the diagnosis of RVH. For these reasons, the diagnosis of RVH using ECG can sometimes be a little bit complicated.
To being, let's look at what RVH would look like in the "precordial" plane:
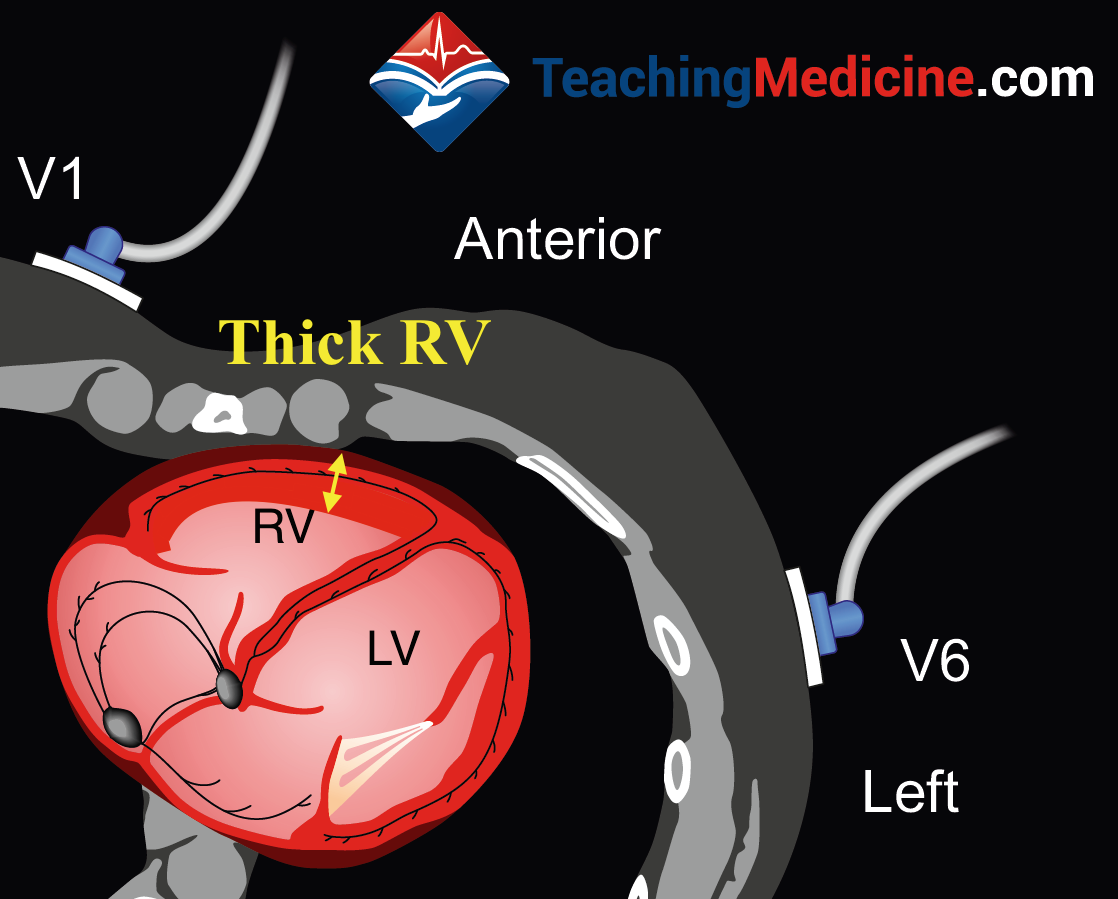
Thick myocardium in this location will result in strong electrical forces directed in an anterior direction, toward V1:
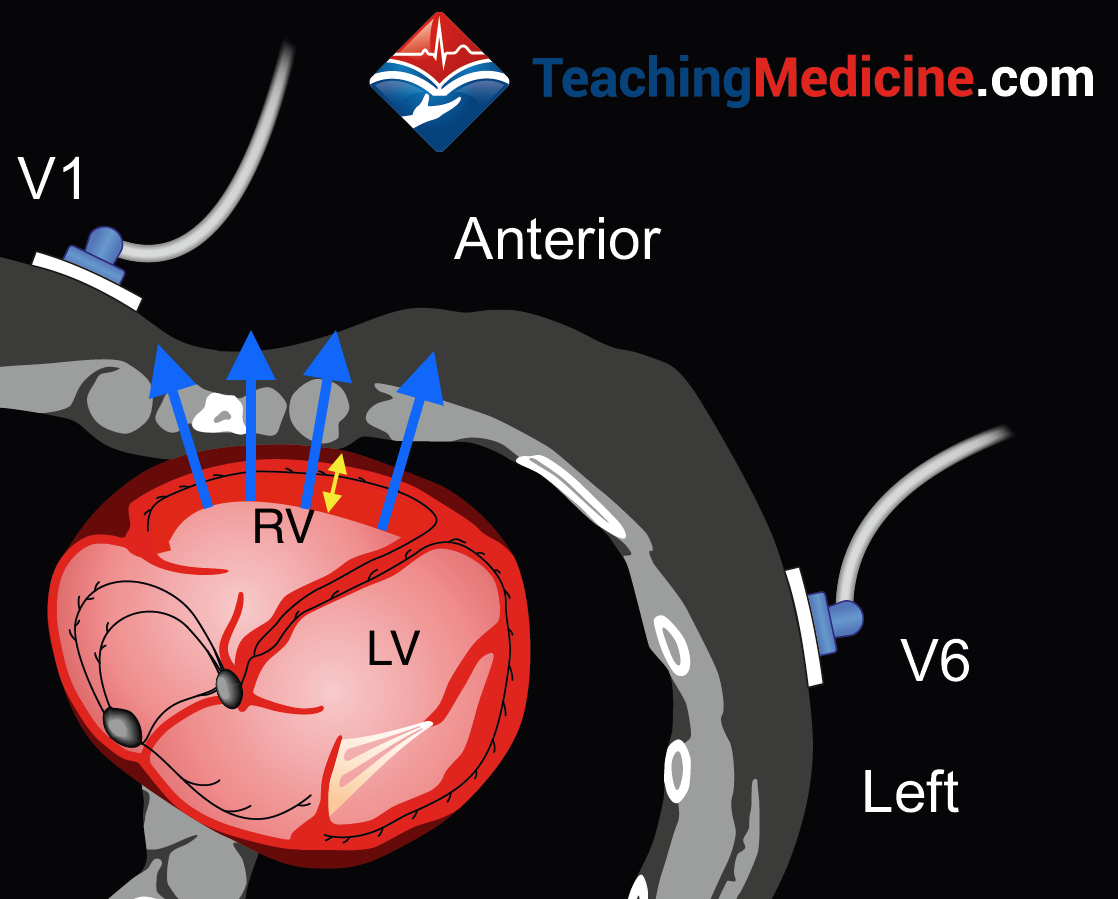
These electrical vectors will create a large upgoing QRS deflection (R wave) in V1 and because they are moving away from V6, they will produce a downward QRS deflection in V6. In a normal ECG, the QRS is mostly downgoing in V1 and upgoing in V6, so this is opposite to normal.
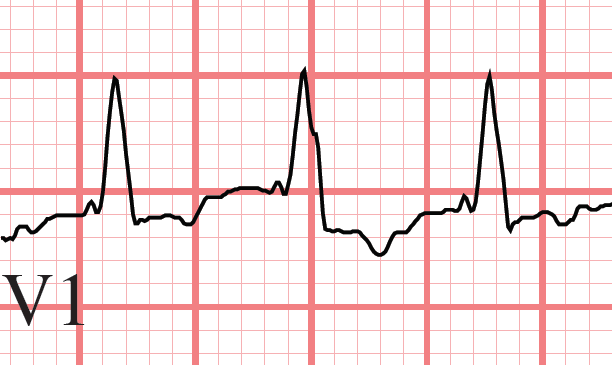
A simple criteria is simply a tall (upgoing) R wave in V1. There are different criteria for what consitutes "tall", but > 6 mm (little squares) is an accepted criteria. The example below is just around 6 mm.
We talk about the R:S ratio for V1. The R is the upgoing part of the QRS deflection and the S is the downgoing part of the deflection. An R:S ratio > 1 means that the QRS is mostly upgoing (the upgoing R is bigger than the downgoing S). An R:S ratio < 1 means that the QRS is mostly downgoing.
In V1 in a normal heart, the R:S ratio is < 1 is normal because the QRS is normally mostly downgoing in this lead.
In RVH, the R:S ratio is > 1 in V1.
Here is an example:
However, other abnormalities can cause R:S ratio > 1 in V1:- right bundle branch block (the rabbit ears, remember?)
- posterior infarct (we haven't covered this yet in our modules)
- WPW (Wolff-Parkinson-White) syndrome (also not yet covered)
- hypertrophy of the septum (can you see how this might happen using the diagram?)
Thus, an R:S ratio > 1 in V1 is suggestive for, but NOT SPECIFIC for RVH. It can be caused by many other things.
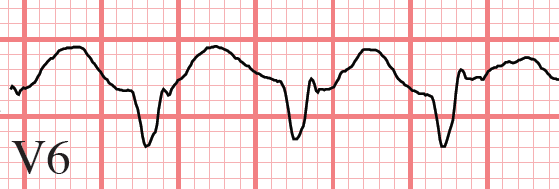
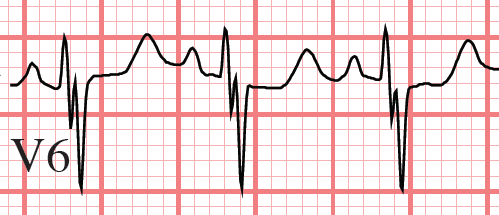
Let's flip this around and look at V6. The electrical forces are moving away from V6 and so we would expect the QRS to be mostly downgoing and therefore have an R:S ratio to be < 1.
RVH causes R:S ratio < 1 in V5 and V6.
Another SUGGESTIVE criteria is right axis deviation (RAD). As a result of stronger electrical forces aiming rightward, the axis will be averaged more to the right. However, RAD can be caused my many things and therefore RAD is not specific for RVH.
RVH is associated with RV pressure overload. If the RV is pressure overloaded, then there is a very high probability that the right atrium (RA) will also be pressure overloaded. Volume or pressure overload of the RA will cause right atrial enlargement (RAE). Therefore, RVH is often associated with RAE.
Summary of diagnostic criteria that SUGGEST the presence of RVH:- tall upgoing R wave in V1 > 6 mm
- R:S ratio > 1 in V1
- R:S ratio < 1 in V6
- right axis deviation (RAD)
- right atrial enlargement (RAE)
It is important to recognize that not all criteria need to be present and that commonly, other abnormalities will be present.
It is also important to recognize that literature on RVH is not unanimous with respect to the diagnostic criteria. In short, ECG is not the best method to diagnose RVH and the criteria are somewhat variable.
