First degree Heart Block Diagnostic criteria: (boldfaced with * indicates an important feature)- Rate: any
- Rhythm: regular
- P waves: all normal
- * PR interval: long (> 5 little squares which is > 200 ms), and constant
- QRS: narrow
Electrophysiology
In first degree heart block, all the P waves are conducted down to the ventricles. In contrast, some but not all the P waves are conducted in second degree heart block (and there are 2 types of second degree heart block) and in third degree heart block, none of the P waves are conducted.The PR interval is comprised of the P wave and the isoelectric segment between the P wave and the QRS which represents conduction through the AV node. Remember that the AV node is small and the electrical signal it produces is so small that we cannot record it from the ECG leads on the skin. This is represented in the image below by the flat purple segment between the P wave and the QRS.
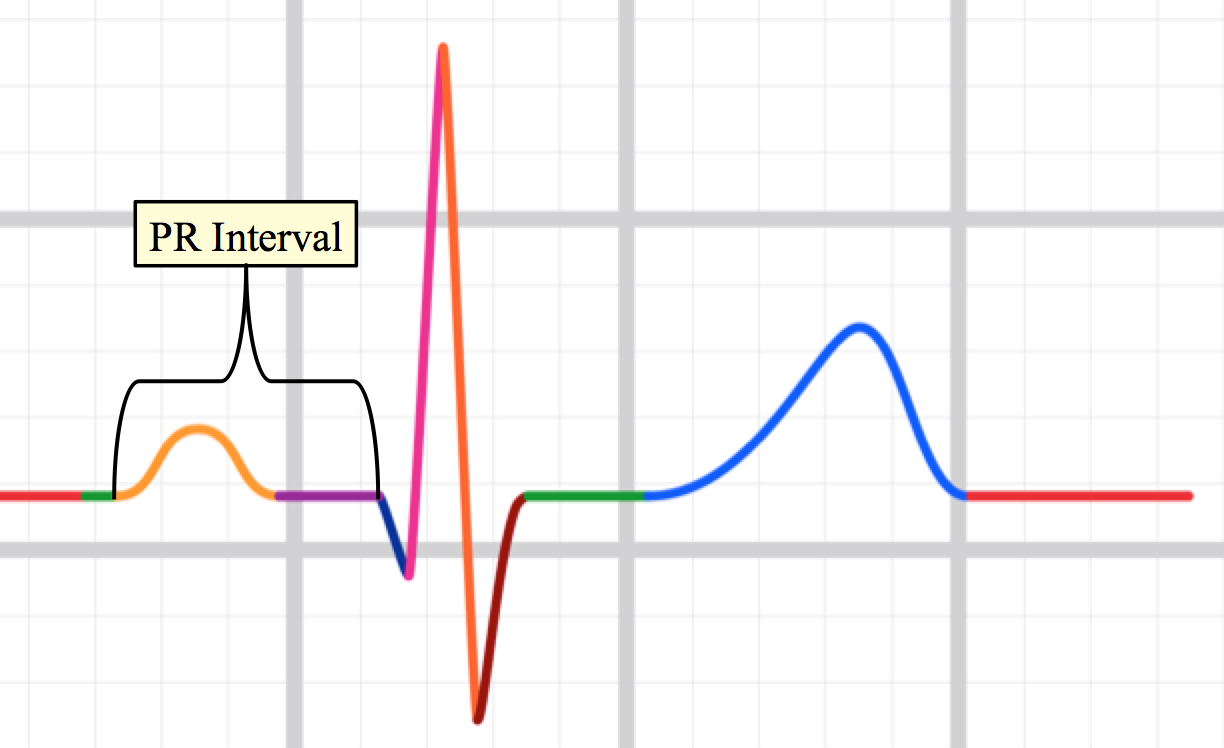
Slow conduction through the AV node will prolong the isoelectric segment between the P wave and the QRS. This will lengthen the PR interval. Conduction through the AV node can be slowed by disease processes (such as ischemia) or by drugs, or by other less common factors.
Clinical Significance:If first degree heart block is the only abnormality of the electrical system, it will have zero impact on the heart rate. It is also very unlikely that the extra delay between atrial contraction and ventricular contraction would have any significant impact on ventricular filling. Therefore, the impact of first degree heart block on blood pressure, heart rate, or cardiac output is negligible.
First degree heart block often occurs when there are other problems in the heart. Therefore, the presence of a first degree heart block should raise the suspicion that there could be other problems with the heart. First degree heart block is associated with atrial fibrillation, meaning that patients with first degree heart block have a higher probability of developing atrial fibrillation compared to patients who do not.
Pacemakers are not recommended for patients with first degree heart block. This is because they do not have a low heart rate (which is what pacemakers are treating) and the probability of a first degree heart block converting to a third degree heart block (which typically does have a low heart rate) is low.
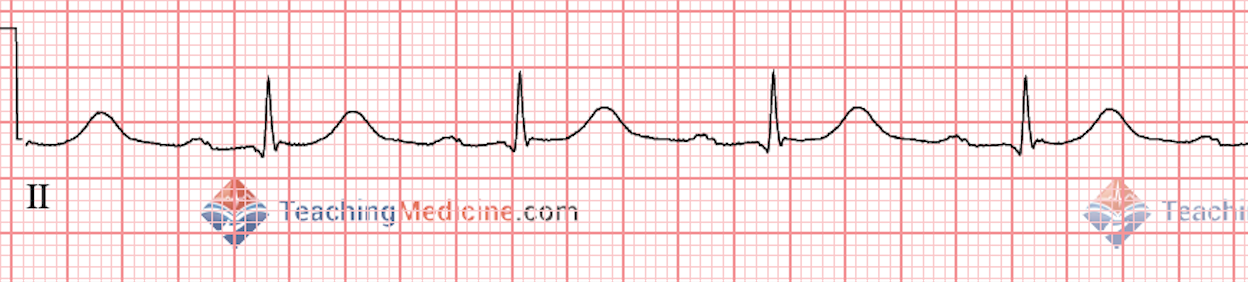
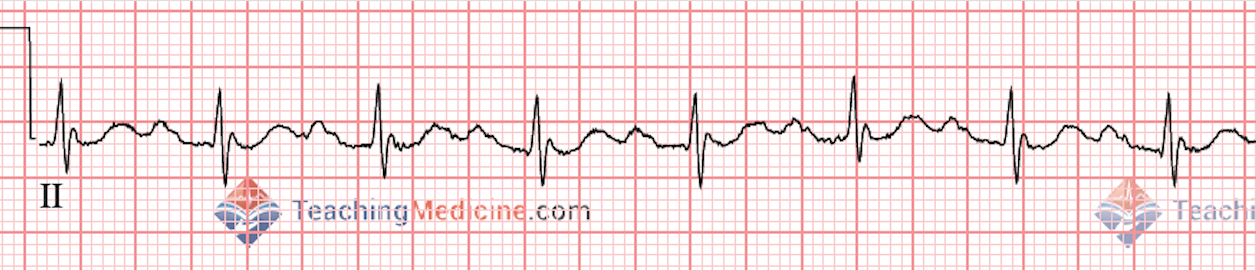
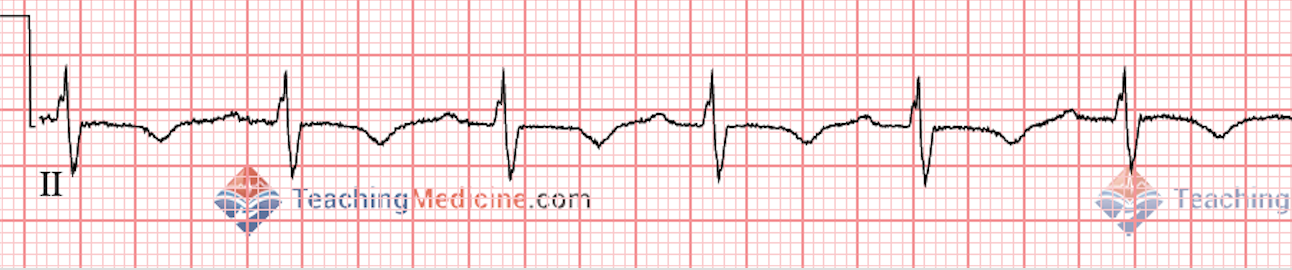
Examples: